First Consensus Meeting on Menopause in the East Asian Region
Menopause and HRT in Malaysia
Nik Nasri Ismail
National University of Malaysia
Introduction
Menopause, which marks the end of reproductive life, characterizes the penultimate stage in a woman’s life. However, this does not signal the end of sexual and social activities. Indeed, the menopause may even be regarded as a blessing by Muslim women, since they are no longer prohibited from participating in religious activities [1]. Although the menopause is associated with symptoms such as vasomotor flushes and psychosomatic symptoms, together with an increased risk of osteoporosis and cardiovascular disease, attitudes and responses to it may differ from community to community. In a study on the menopausal situation in Malaysia, the mean age of menopause was found to be 50.7 years [2]. In a previous study several years ago, the mean age was 48.7 years [3]. Both findings are within the range documented in most industrialised societies. A biological phenomenon which was not a topic much talked about before in Malaysia, menopause is now more frequently discussed due to better availability of information, but more so due to the fact that the average life expectancy of Malaysian women has increased from 68 years in 1985 to 74 years in 1993, i.e. one-third of the average Malaysian woman’s life will take place in the postmenopausal period.
Endocrinology of menopause
Menopause is characterized by fairly drastic changes in the hormonal milieu. The sole primary endocrine phenomenon of menopause is the decrease of ovarian follicular production of oestrogens. Through an active feedback on the hypothalamo-pituitary tract, this results in increased production of gonadotrophins. The level of oestrogens decreases to about one-fifth of the premenopausal level. Postmenopausally, circulating oestrogen levels consist mainly of estrone, which has one-sixth of the potency of estradiol, the predominant premenopausal oestrogen (mean levels 100-200 pg/ml of estradiol in menstruating women).
In the postmenopausal woman, the mean level of oestrogens is 45 pg/ml, consisting mainly of estrone. The main source of oestrogens in the postmenopausal woman is the peripheral conversion of androstenedione to estrone in the adrenals glands. This process of aromatization also occurs in the liver and in adipose tissues; this is why adipose women complain of less menopausal symptoms, genital atrophy and osteoporosis. On the other hand, they have a higher risk of developing endometrial cancer. The postmenopausal ovaries, however, continue to produce testosterone in the stromal tissues.
The decrease of oestrogen levels, causing an active feedback on the hypothalamo-pituitary tract, leads to an increased production of gonadotrophins (FSH = follicle-stimulating hormone, and LH = luteinising hormone). The decrease in oestrogen levels is initiated some years before the actual menopause, causing irregular bleeding in the perimenopausal woman. Thus, in women still having their periods and complaining of menopausal symptoms, it is necessary to measure hormone levels. From a biochemical viewpoint, the actual menopause may be diagnosed after cessation of menses for longer than 12 months along with 17b-estradiol levels < 74 pmol/l and FSH levels > 30 IU/l.
The reduction of oestrogen levels results in atrophy of the vulva, vagina, ovaries, tubes and the breasts. Together with a dry, coarse skin and some degree of hirsutism, the atrophy of the genital tract causes a decrease in femininity and sexuality. The shorter, thinner and dry vagina can lead to dyspareunia which may cause marriage breakups. Because of their high concentration of oestrogens receptors, there is also atrophy of the bladder and the urethra, causing symptoms like urgency, stress incontinence, frequency and nocturia. The weakened ligaments and tissues of the genitalia can also result in uterovaginal prolapse.
The Malaysian community
Malaysia is a cosmopolitan country. There are three main ethnic groups: Malays (50%), Chinese (30%), Indians (15%), and several minor ethnic groups (5%). The Malaysians today live happily intermixed between the various ethnic groups. The country’s population in 1995 was 23 million and is expected to be 32 million by the year 2020, the year that Malaysia hopes to be recognised as a developed country. By 2020 also, 6.6% of the population will be older than 65 years, as compared to 2.3% now. A better health care system, better nutrition and a better environment contribute to this increase in life expectancy among the Malaysians.
Age of menopause
In 1989, Arshat et al. [4] conducted a survey among women in two rural areas and estimated the age of menopause to be 48.7 years. The majority of women in the study were Muslim Malays. In 1990, Nik interviewed 400 women aged 40-60 years. The study population consisted of 70% Malays, 13% Chinese and 17% Indians. Most of these women were interviewed in their homes, but some were interviewed at the supermarket or in shopping malls. As permitted by the study protocol, 10% (n = 40) were either patients of gynaecological and antenatal clinics or nursing staff at the hospital. These women were living in the urban area of Kuala Lumpur, the capital city. It was observed that the median age at menopause was between 50 and 51 years (50.7). However, both ages (48.7 and 50.7) were within the range of menopausal age documented in most industrialised countries.
Sociodemographic profile of menopausal women
The distribution of the 400 patients according to age is shown in Table I, the distribution being more or less even up to the age of 55 years. There were only six patients beyond that age. The majority (76%) of these women were still married and living with their husbands.
Table I: Age distribution (n = 399)

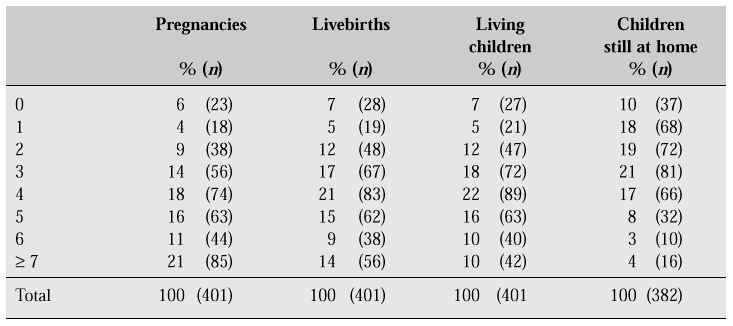
Sixty-one percent (61%) of the sample were married before the age of 20 years (Table II). Eighteen percent (18%) of the sample reported having three living children, 22% four children, and 36% five and more children (Table III). Unlike the situation in Western countries, it is quite usual to have many children in a family. Fifteen percent (15%) of the women reported still having five or more children living at home with them. About a quarter (27%) even had their grandchildren staying with them in an extended family system.
Table II: Age at marriage (n=355)

Table III: Pregnancies, livebirths, living children and children still at home
Forty-nine percent (49%) of the study population had the basic 5-6 years of primary education. Only 8% had university level education, while the remainder (23%) had received education for 9-12 years. As regards their social position, 50% of the women in the sample were working full time, 5% were on a part-time basis and 37% had no other job except the important one of full-time housewife.
By the age of 15 years, 90% of the women investigated had reached menarche (Table IV), while for 10% (n = 40) menarche occurred at 16-17 years of age.
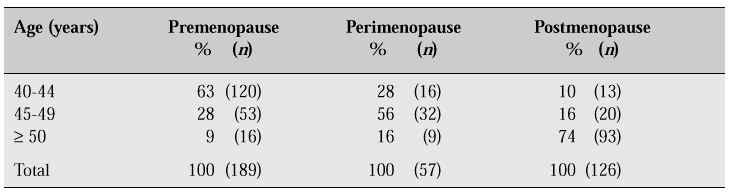
Table V shows the relationship between age and menopausal status. Fifty-one percent (51%) of the sample were premenopausal, 15% perimenopausal and 34% postmenopausal. The median age at menopause was between 50 and 51 years of age (50.7)
Table IV: Age at menarche (n = 397)
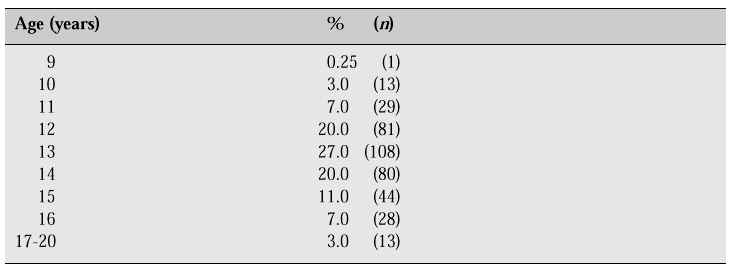
Table V: Age and menopausal status
Symptoms and complications
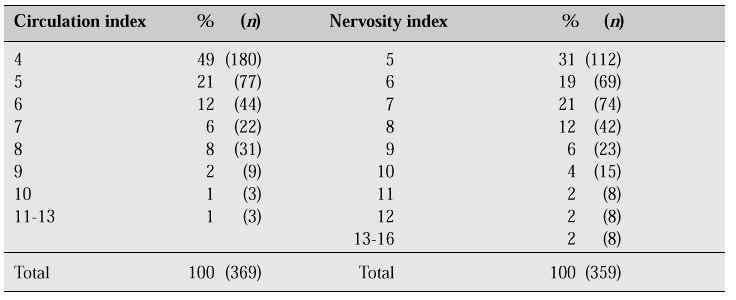
From the circulation and nervosity indices, it is apparent that the Malaysian women studied in 1990 did not suffer from serious menopausal symptoms (Table VI).
Table VI: Circulation index (hot flushes, sweats, palpitations, dizziness) and Nervosity index (irrita-bility, headache, depression, insomnia).
This could be attributed to the hot weather prevailing the whole year round (average temperature of 26¡C - 28¡C) as well as to ignorance of vasomotor symptoms. After all, there was no menopause clinic set up anywhere in the country, although gynaecologists were seeing menopausal women as part of their general gynaecology clinics patients. Thus we saw that more than 70% of the study population reported never having had symptoms like hot flushes, sweating or palpitations (Table VII). The incidence and severity of climacteric symptoms depend mainly on the presence of emotional instability before menopause [3,4]. An earlier study in 1986 found that less than 20% of respondents were symptomatic [2].
Table VII: Symptoms according to menopausal status
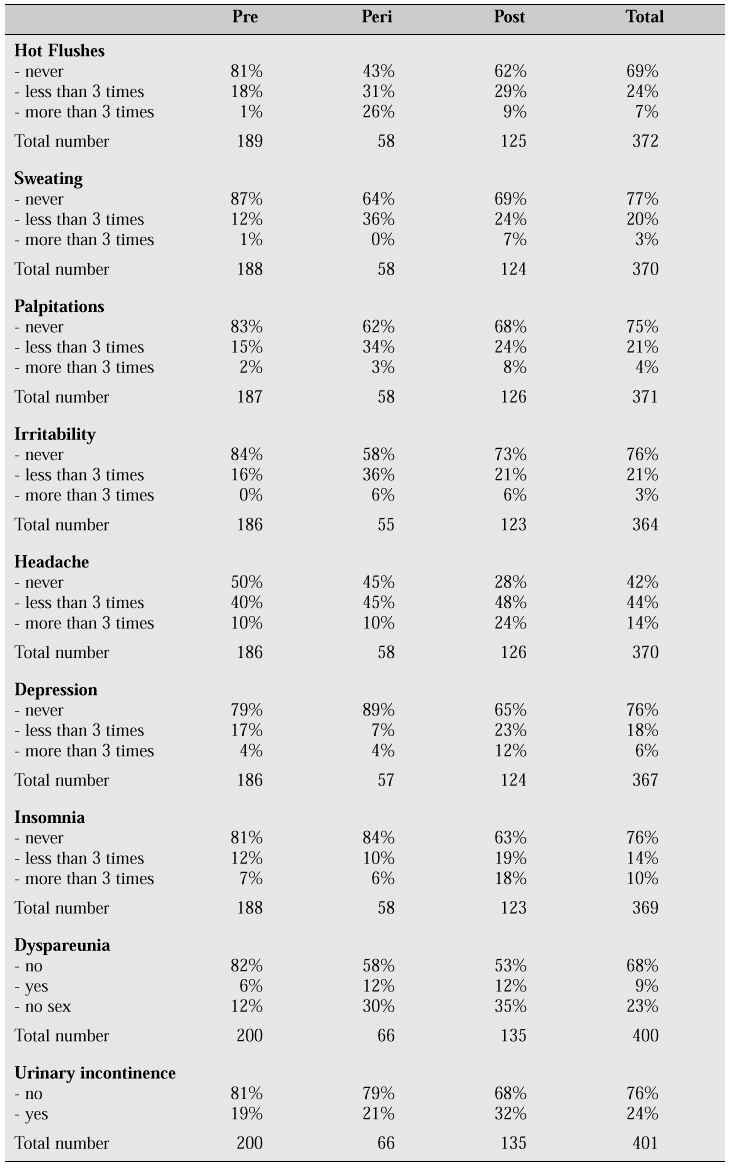
Analysis of the climacteric symptoms reported showed that it was in the perimenopausal group that most of these symptoms occurred, (peri- > post - > premenopausal): 57% reported hot flushes on a scale from < 3 >3 times/day, 36% reported night sweats < 3 times/day, 34% reported palpitations < 3 times/day, meaning that in general the symptoms are perceived as being mild.
It can thus easily be understood why 80% of the three ethnic groups saw no real reason to consult a doctor. Educational level and having or not having a job exerted no influence in this respect. Of those who consulted a physician for medical advice, 84% (n = 58) were given some form of prescription - for hormones (31%), tranquilizers (28%), herbal medicines (41%), etc. - but almost half (43%) decided not to comply with the prescription they were given.
When asked about dyspareunia, 68% claimed that they had no problems and only 9% thought they suffered from this condition, while 23% had ceased sexual activity for various reasons. Among the women suffering from dyspareunia, less than 20% had consulted a physician. Malaysian women then were not ready to discuss sexual difficulties after menopause unless the discussion were to be initiated by the attending doctor.
Finally, only 24% of the women in the sample complained of urinary incontinence, but again the majority of these (82%) preferred not to discuss their problem with a doctor. It is therefore not surprising that 80% of the sample rated their health as ‘good’.
Menopause clinics in Malaysia
In 1989, the Family Planning Federation of Malaysia tried to set up a Mature Women’s Clinic, and in 1990 the Well - Women’s Clinic, to cater for menopausal women. Both attempts failed since no women came forward. However, when the first special menopause clinic was launched in July 1991, Malaysian women with menopausal complaints at last found the place to approach for counselling and hormone replacement therapy (HRT). This was in Kuala Lumpur, the capital city. Today, through continuing medical education programmes, several other menopause clinics have been set up in many other parts of the country, both in government hospitals and in private medical centres. Pharmaceutical companies and professional organisations are actively helping to publicize the knowledge regarding menopause and HRT. As from February 5th, 1997, the Malaysian Menopause Society has been established.
Selection of patients for HRT
HRT is being offered to most oestrogen-deficient women, although the greatest benefits would be for those with natural or surgical menopause symptoms, those with osteoporosis or those at risk of cardiovascular disease or osteoporosis. However, before initiating anyone on HRT, it is mandatory that the woman should be examined thoroughly after taking a complete history. Special attention should be paid to prior personality disorders, psychological problems, psychiatric disorders, interpersonal relations, menstrual history, surgical problems and associated symptoms. Weight, height and blood pressure must be measured and the breasts and pelvis examined.
All new cases should be subjected to the following investigations and followed serially or as and when indicated:
1. Pap smear for those with uterus
2. Fasting lipid profile
3. Mammography
4. Fasting blood sugar
5. Urinary pyridinium crosslinks for bone turnover assessment
6. Others if indicated — endometrial biopsy, FSH, LH, ultrasound
Choice of therapy
This depends on whether the woman has a uterus or not. In principle, women who still have their uterus would be given HRT, i.e. a combination of oestrogen and progestogen, while those without uterus can be given ERT, i.e. oestrogen only. Various forms of HRT are currently available — tablets, gels, patches, creams and implants. Very recently, herbal therapy has become available for women with vasomotor symptoms but with a contraindication for HRT.
Depending on the choice of the individual patient, there is a therapy causing a monthly withdrawal bleeding or the more popular non-bleeding continuous therapy. The women are free to choose and decide to ensure compliance to therapy.
Conclusion
In conclusion, the median menopausal age of Malaysian women is around 50.7 years, which is well within the range documented in most industrialised societies [5,6]. The biological phenomenon of menopause was not a topic to be talked about in Malaysia, but is now a much discussed topic among professional and non-professional organisations. With the setting-up of more menopause clinics, Malaysian women can look forward to living their extended life expectancy with happiness and zest.
References
1. Khalid BAK. The postmenopausal woman. AFES 1987; 6:27-32.
2. Seng CK. Menopause. Okura; 1986.
3. Weideger P. Female cycles. London: The Women’s Press; 1978.
4. Arshat H, Tey NP. Ramli N. (1989). A study on age at menopause and menopausal symptoms among Malaysian women. Malays Reprod Health 1989; 7:1-9.
5. Reitz R. Menopause, a positive approach. London; UNWIN; 1979.
6. Frommer DJ. Changing age of menopause. Br Med J 1964; 2:349.